
FORM 1
EP 1110-1-29
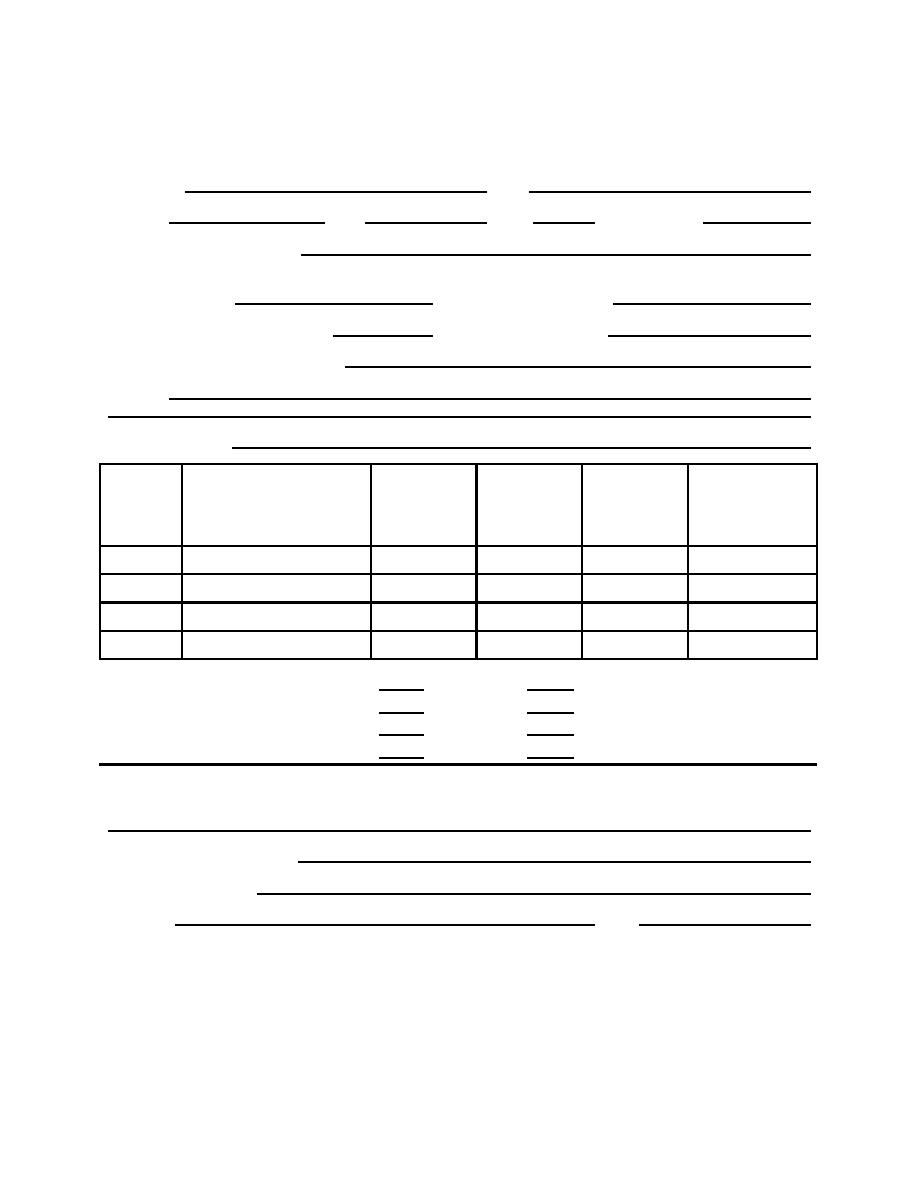
LEAD HAZARD CONTROL VISUAL CLEARANCE FORM
31 Aug 01
Installation:
POC:
Address:
City:
State:
Housing Group:
Abatement Method/Treatment:
Date/Time
Date/Time
Cleanup Completed:
Inspection Initiated:
Check if repeat clearance inspection:
Date of initial inspection:
Lead Hazard Control Contractor Name:
Address:
Telephone Number:
Work on each
Visible paint
Room
List all building components
Visible settled
component
chips/waste or
Additional work
Name and
required to be treated in each
dust seen
completed
debris seen
required
Number
room
(yes or no)
(yes or no)
(yes or no)
Exterior soil
Treated
Not treated
If treated, is bare soil present?
Yes
No
Was contaminated soil removed?
Yes
No
Is additional soil treatment required?
Yes
No
NOTES:
Name of Risk Assessor (print):
Certification Number(s):
Signature:
Date:
Figure C-1: Lead Hazard Control Visual Clearance Form
C-2
Page ___of___

 Previous Page
Previous Page
